On Saturday, February 24, another case of measles was reported in Florida, making it the seventh in the state, and the first one outside the Manatee Bay Elementary school in Weston, Fl where 6 students were reported to have contracted the disease that same month. This case reported in the Ft Lauderdale area was in a young child not associated with the aforementioned school, but does raise questions about how this new case arose. Weston and Ft. Lauderdale are approximately 20 miles apart and transmissibility in measles is extremely high.
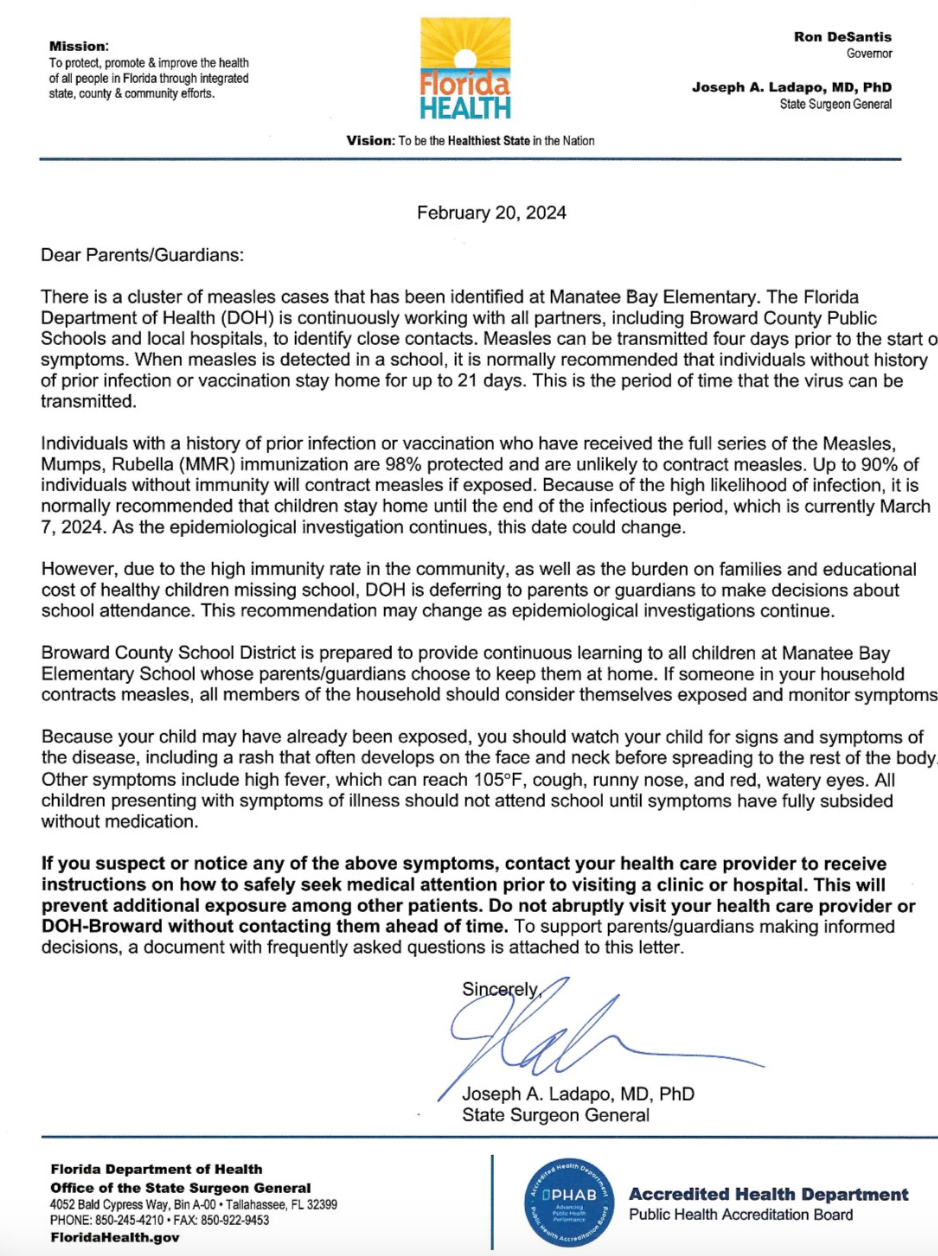
Just days before, on February 20, the Florida Surgeon General Joseph Ladapo, MD, PhD, sent out a letter to address the ongoing outbreak at the school. In the letter, Ladapo left the decision about sending children to school to the parents.
In the letter, it stated: “When measles is detected in a school, it is normally recommended that individuals without history of prior infection or vaccination stay home for up to 21 days. This is the period of time that the virus can be transmitted.
Individuals with a history of prior infection or vaccination who have received the full series of the Measles, Mumps, Rubella (MMR) immunization are 98% protected and are unlikely to contract measles. Up to 90% of individuals without immunity will contract measles if exposed. Because of the high likelihood of infection, it is normally recommended that children stay home until the end of the infectious period, which is currently March 7, 2024. As the epidemiological investigation continues, this date could change.
However, due to the high immunity rate in the community, as well as the burden on families and educational cost of healthy children missing school, DOH [department of health] is deferring to parents or guardians to make decisions about school attendance. This recommendation may change as epidemiological investigations continue.”
In the entire letter, posted below, there is no mention of families getting the MMR vaccine if they have not already or been exposed to measles.
The letter sent by Florida Surgeon General Joseph Ladapo, MD, PhD after the measles outbreak in the state.
This public health messaging might be confusing to families if their children have not had measles or have not been vaccinated against it, especially when they are deciding if their children should quarantine or take their chances of sending their kids to school. This communication disconnect between public health and families is a major ongoing issue, and in the background of COVID-19 vaccine disinformation and misinformation, it just leaves everyone with an uncertainty and can lead to a dangerous inertia.
Measles Transmissibility
Measles is spread by breathing in contaminated air or touching an infected surface then touching the eyes, noses, or mouths. According to the Centers for Disease Control and Prevention (CDC), the measles virus can live up to 2 hours in airspace after an infected person leaves an area and can linger on surfaces for hours. And, if you put a person with measles in a room with 10 people who have not been vaccinated or have not previously contracted measles, 9 of those people will also get the disease.1
“Measles is the most contagious and easily transmittable virus we know—far more than COVID or influenza,” said Patricia A. Stinchfield, RN, MS, CPNP, president, National Foundation of Infectious Diseases (NFID).
During her career as a pediatric nurse practitioner, Stinchfield has treated numerous measles cases. In fact, she oversaw 3 outbreaks, and says that when young children come in with disease, they are “some of the sickest children.”
“They will come in very dehydrated. They are photophobic, and their eyes hurt and are very red. They need to stay in a dark room. They need IV fluids, they have severe diarrhea, and often they’ll have otitis media or ear infections.”
In addition to these typical symptoms, there can be severe disease that can lead to bad outcomes.
“They often will have pneumonia and that is the reason that people succumb to measles—both viral measles pneumonia in the lungs itself and then secondary bacterial infection,” stated Stinchfield. “So 1 in 5 unvaccinated people who get measles will get hospitalized. And 1 in 20 children with measles will get this pneumonia described…One in 1000 who get measles will develop a severe encephalitis that they might survive. Everyone talks about well, very few people die of measles, but even those who survive it, they can get this encephalitis and develop seizures.”
Despite these statistics, measles outbreaks have been occurring all over the United States this year. CDC states that 35 cases of measles were reported in 15 states including Arizona, California, Florida, Georgia, Indiana, Louisiana, Maryland, Minnesota, Missouri, New Jersey, New York City, Ohio, Pennsylvania, Virginia, and Washington.2
A Reduction in Vaccine Rates
CDC reports there has been a trend showing a reduction in children getting their standard immunizations. In January 2023, the CDC reported that over the last 2 school years, the national coverage for childhood state-required vaccines among kindergarten students declined from 95% to approximately 93%. During the 2020-21 school year, vaccinations dropped to 94% and during the 2021-22 school year it dropped again to approximately 93%.3
And while this does not sound like a large number, it still represents thousands of young children not getting their vaccinations. It is also a disturbing trend as some families may feel they do not need them or are fearful of vaccines.
“Compared with the 2020–21 school year, vaccination coverage decreased 0.4–0.9 percentage points for all vaccines. Although 2.6% of kindergartners had an exemption for at least 1 vaccine, an additional 3.9% who did not have an exemption were not up to date with MMR,” the investigators wrote in an MMWR last year.3
This is the lowest rate of vaccination in over a decade, the CDC states. And the MMWR report said that as many as 250,000 kindergartners are not protected against measles.3
There were more than 1200 cases of measles reported in the United States in 2019—the highest number in decades. In 2022, there was 121 cases of measles.2 In 2023, there was a substantial outbreak in Ohio and Kentucky that had 85 children contract the disease, and 35 of them were hospitalized.3
“The short answer is measles vaccination rates are too low; The long answer is when those rates go below 95%—and this is really about in a specific community…When a local community gets below 95%, that gives measles an ability to make an entrance and spread in that community,” Stinchfield said. “So we always have vulnerable people to measles; we always have babies too young to be immunized; we always have immunocompromised people; [we have] people on various therapies that make them vulnerable to measles…even when our rates are high, we’ve got people that will always be susceptible to measles.”
“Despite the care taken in the development and deployment of vaccines and their clear and compelling benefit of saving individual lives and improving population health outcomes, an increasing number of people in the US are now declining vaccination for a variety of reasons, ranging from safety concerns to religious beliefs,” wrote FDA Commissioner Robert Califf, MD, and Peter Marks, MD, director of the Center for Biologics Evaluation and Research in a viewpoint article in a recent JAMA.5
Vitamin A for Measles Treatment
In terms of treatment, there haven’t been any FDA approved medical therapies to relieve symptoms; however, vitamin A has been identified as a treatment for measles.
“All children or adults with measles should receive 2 doses of vitamin A supplements, given 24 hours apart. This restores low vitamin A levels that occur even in well-nourished children. It can help prevent eye damage and blindness. Vitamin A supplements may also reduce the number of measles deaths,” WHO writes on its site.4
It is underutilized as a treatment in the United States. Back in 2019, NFID convened a summit and discovered that in the US less than 50% of hospitalized patients were being treated with vitamin A. As a result, NFID developed a report, Call to Action, Vitamin A for the Management of Measles in the US, with recommendations on using vitamin A for measles treatment.
“Once someone has measles, vitamin A should be prescribed to patients…And we would encourage clinicians to take a history of their vitamin A, making sure they weren’t taking a lot of vitamins prior to their infection,” Stinchfield said. “It’s an important tool to manage and to start promptly. So, clinicians and pharmacists should look at this tool and know what the doses are. They’re very age specific doses. You should have the vitamin A on hand, and ready to go—and it’s in amounts that would normally not be carried by pharmacies.”
Reducing Incidence Rates
While it is not optimal, there is still some benefit to getting the MMR vaccine, post-exposure. For those who have been exposed to measles, and have not been vaccinated or contracted it, Stinchfield explains time is of the essence when it comes to getting the vaccine, saying there is a 72 hour window from exposure. The results of these vaccination interventions can be quite good.
“Children who have been exposed and got their MMR vaccine within that 72 hours can go back to daycare and school, because we feel that they have that protection and coverage that they need,” Stinchfield said. “If you miss that 72 hour window, for some people there is measles immune globulin that can be recommended.”
In terms of trying to reduce incidence rates overall, Califf and Marks point to the significant trust the public has with clinicians and retail pharmacists, but that everyone in the medical field has a role in educating the public.
“All those working in health care, while being straightforward about the risks, need to better educate people regarding the benefits of vaccination, so that individuals can make well-informed choices based on accurate scientific evidence.”5
Contagion will be publishing the video portion of the interview with Stinchfield in the coming days.
References
1.Measles. Transmission. CDC. Last reviewed November 5, 2020. Accessed February 28, 2024.
https://www.cdc.gov/measles/transmission.html
2. Measles. Cases and Outbreaks. CDC. Last reviewed February 23, 2024. Accessed February 28, 2024.
https://www.cdc.gov/measles/cases-outbreaks.html
3. Parkinson J. Measles Outbreak in Philadelphia Prompts Caution, Calls for MMR Vaccination. ContagionLive.com. January 8, 2024.
https://www.contagionlive.com/view/measles-outbreak-in-philadelphia-prompts-caution-calls-for-mmr-vaccination
4. Measles. WHO. August 9, 2023. Accessed February 29, 2024
https://www.who.int/news-room/fact-sheets/detail/measles
5. Marks P, Califf R. Is Vaccination Approaching a Dangerous Tipping Point? JAMA. Published online January 05, 2024. doi:10.1001/jama.2023.27685